
|
COPD
|
|
|
Features
|
· Both emphysema and chronic bronchitis are manifestations of COPD.
· Pulmonary function tests show obstructive physiology (reduced FEVI/FVC, increased RV and TLC)
· DLCO is normal in chronic bronchitis and decreased in emphysema.
|
|
S/S
|
SOB – Productive Cough
|
|
Dx
|
Clx –> PFT
|
|
Tx
|
Stable pt:
1˚ Ipratropium
2˚ Albuterol (may precipitate HF through ⤴️ HF)
3˚ Theophyline
–Stop smoking
-Home O2 (Start if: PaO2 <55 / O2 <88%)
-Vaccine: Pneumococcus q5 ys / Flu q1y
Exacerbation 🚨
· Get: O2 Saturation + ABG + CXR
· Give O2
· Ipratropium + Albuterol TOGETHER
· Systemic Corticosteroids (PO = IV)
· ABx
If pt is on theophylline → check levels & DON’T D/C!
|
|
Acute Exacerbation of COPD
|
|
|
S/S
|
· ⤴️ SOB
· ⤴️ Cough (more frequent or severe)
· Sputum (change in color or volume)
|
|
Dx
|
CXR: Hyperinflation
ABG: Hypoxia, C02 retention (chronic &/or acute)
|
|
Tx
|
· Oxygen (target Sp02 of 88%-92%)
· Inhaled bronchodilators
· Systemic GCS
· Abx if? ≥2 cardinal sx
· oseltamivir if? evidence of influenza
· Non-invasive positive pressure ventilation if ventilatory failure
· Tracheal intubation if NPPV failed or contraindicated
|
|
Asthma
|
|
|
Features
|
Reversible AW obstruction
|
|
S/S
|
Acute AW obstruction w/ SOB & Wheezing
|
|
Dx
|
· Clx → PFT (Gold standard)
· CXR: ⓝ
|
|
Acute Exacerbation
Tx
|
· 1˚ O2 / SABA / ipratropium?
· 2˚ IV methylprednisone
· 3˚ (no improvement w/i 1 h) Mg
· non-invasive positive pressure
· If iminent resp failure → ICU + Intubation
· If pt has ⓝ/⤴️ PaCO2
· Muscle fatigue
· ⤵️ Breath sounds
· Hypoxia
· AMS
|
|
Chronic Tx
|
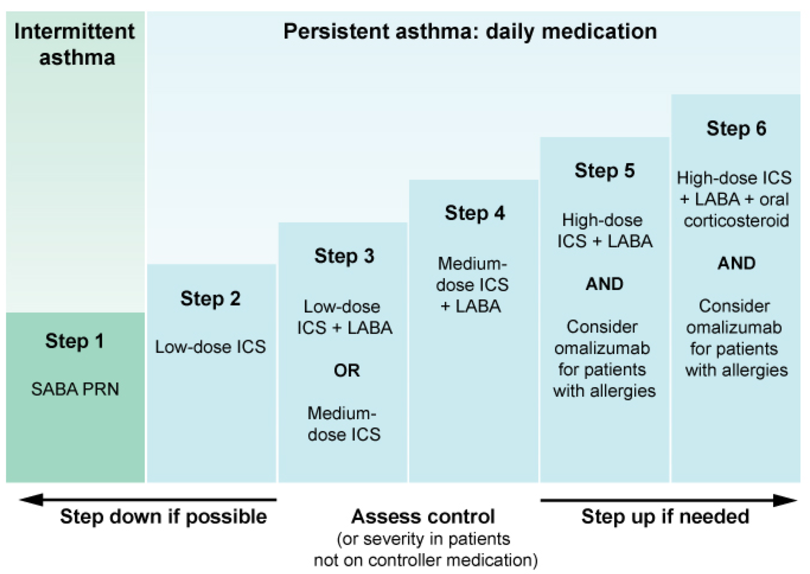 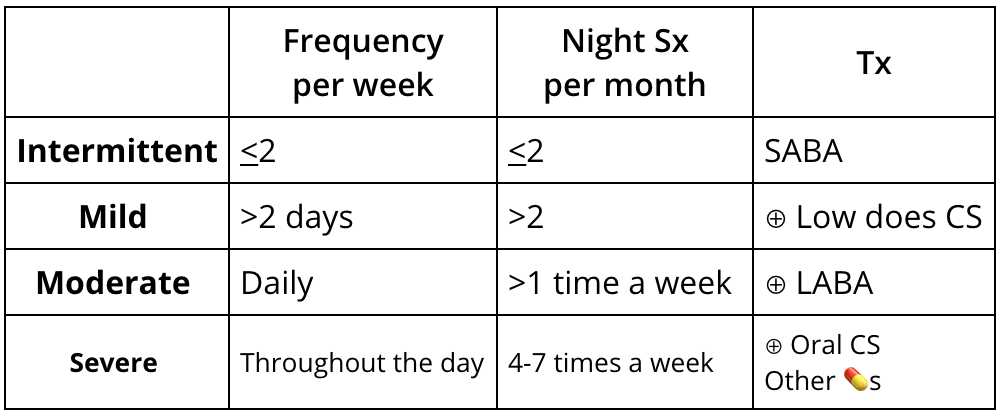 |
|
Bronchiectasis
|
|
|
Pathology
|
· Recurrent infections + Impaired clearance
· That leads to bacterial overgrowth & Nø infiltration → tissue damage & AW structural changes
|
|
Causes/RF
|
· AW obstruction (Cancer)
· Aotuimmune (RA, Sjögren),
· Chronic infection (Aspergillosis, mycobacteria)
· Immunodeficiency (Hypo-Ig)
· Congenital (Cystic Fibrosis, alpha1-antitrypsin deficiency)
|
|
S/S
|
· chronic daily cough
· ⊕ a lot of pus produced
· Rx Rhinosinusitis, SOB, hemoptysis
· Crackles, wheezing
|
|
Dx
|
· High Resolution CT scan of the chest (needed for initial diagnosis)
· Immunoglobulin quantification
· CF testing, sputum culture (bacteria, fungi & mycobacteria)
|
